
Trending Now
- The Central Govt has already released the Rs.1,000 crore we requested for the Disaster Management Department. The funds were provided in advance as a precautionary measure.” – Minister Sengottaiyan
- “There are unannounced power cuts even in Perambur, the constituency of CM Vijay. The TVK Govt says one thing and does something else.” – T.T.V.Dhinakaran
- “We are openly informing about the causes of power outages and how long it will take to fix them” – Minister Nirmal Kumar explains
- CM Vijay will be traveling to Delhi tomorrow and is reportedly expected to meet Rahul Gandhi and Sonia Gandhi.
- “If the TVK Govt falls, we are ready to face a fresh election. Is the DMK ready?” – Minister Arunraj
Coimbatore

A New Era in Cardiac Pacing: Lead to Leadless- Implantation of the World’s Tiniest Dual-Chamber Leadless Pacemaker at PSG Hospital

![]() May 20, 2026
May 20, 2026

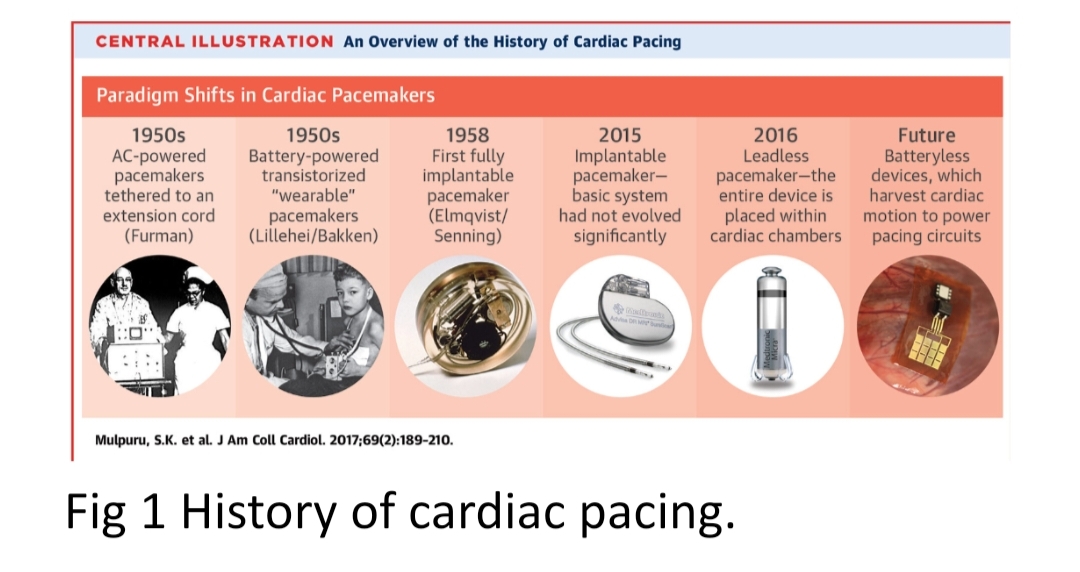
Cardiac pacing has undergone a remarkable transformation over the past few decades, from the 1950s to the present era, evolving from bulky external pacing systems to highly sophisticated minimally invasive technologies as in Fig 1. Conventional pacemakers, though lifesaving, require the implantation of a pulse generator within a surgically created pocket along with transvenous leads that pass through the veins into the heart. While effective, these systems may be associated with complications such as pocket infections, lead fractures, venous thrombosis, lead displacement, and long-term device-related morbidity and are still considered the Achilles’ heel of this rhythm-control therapy.
The leadless permanent pacemaker system was developed as an option to bypass the weakness of the transvenous approach. Advances in battery technology and deep miniaturisation of electronics now offer the opportunity to implant the whole pacemaker system into the right ventricle
The advent of leadless pacemakers represents a revolutionary advancement in modern cardiac electrophysiology. These miniature self-contained devices are implanted directly inside the heart using a catheter-based minimally invasive technique, thereby eliminating the need for surgical pockets and transvenous leads. Their extremely small size, lower infection risk, improved cosmetic outcome, faster recovery, and reduced lead-related complications have made them one of the most significant innovations in contemporary cardiology.
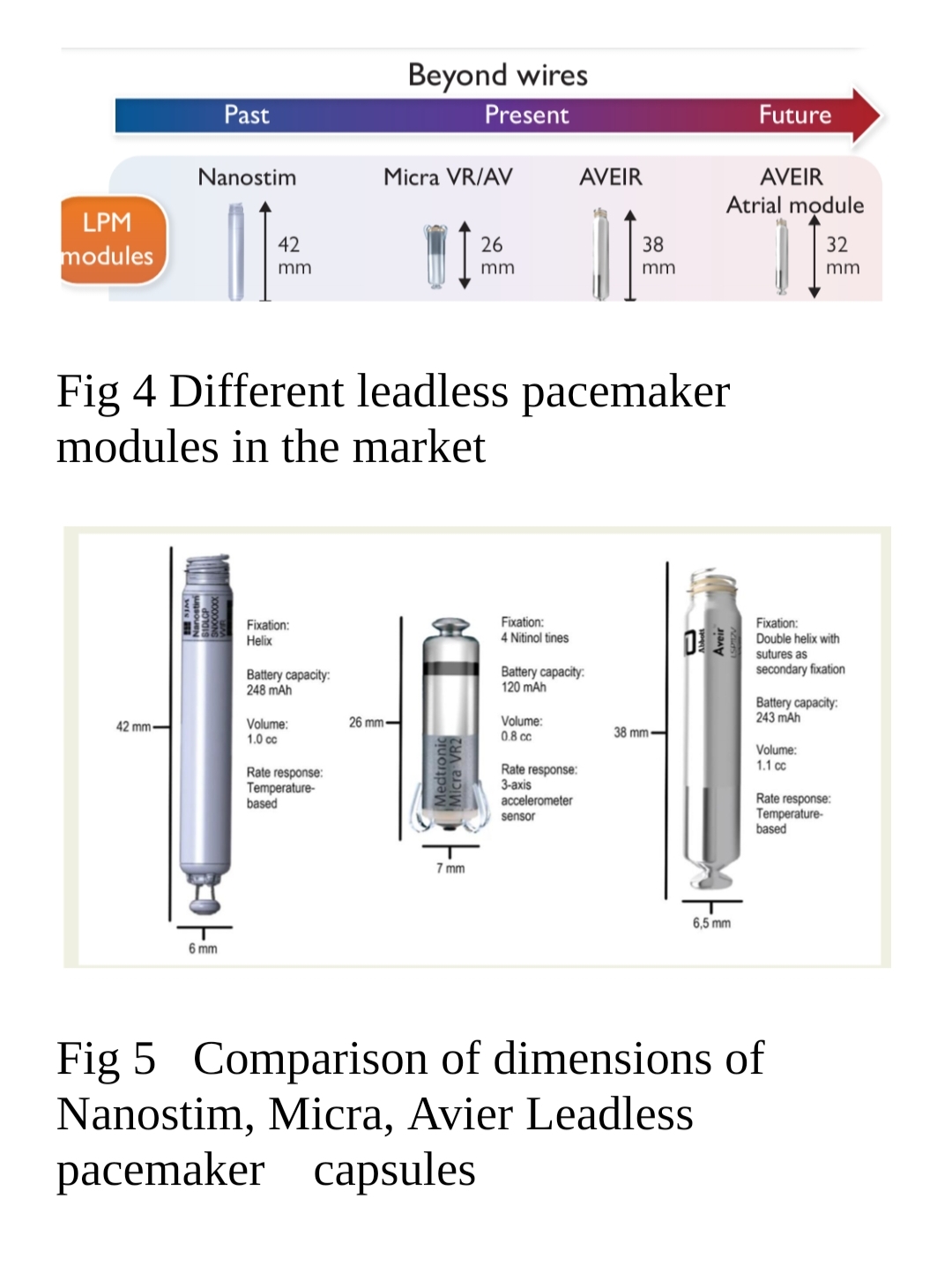
First introduced in 2012, three different Leadless pacemakers (LPMs) have been introduced: the Nanostim LPM (St. Jude Medical/Abbott, Chicago, IL, USA), the Micra transcatheter pacing system (Medtronic, Minneapolis, MN, USA), and the AVEIR LPM (Abbott) shown in (Fig 4,5,6). The first LPMs were limited to a selective group of patients, who only required ventricular pacing in VVI(R) mode. To enlarge this selective patient population, the next generation of LPMs was introduced offering atrioventricular (AV) synchronous ventricular pacing (Micra AV) as in fig 7. Recently, the first dual-chamber LPM (AVEIR DR) (fig 6) is available offering all pacing modes including AAI(R), VVI(R), and DDD(R), but at a much higher cost compared with conventional pacemakers.
The recently introduced dual-chamber leadless pacing system AVIER LPM from Abbott further represent a major leap in cardiac rhythm management by enabling physiological atrioventricular synchrony while maintaining the benefits of a completely leadless system.
Common Indications for Leadless Pacemaker Implantation
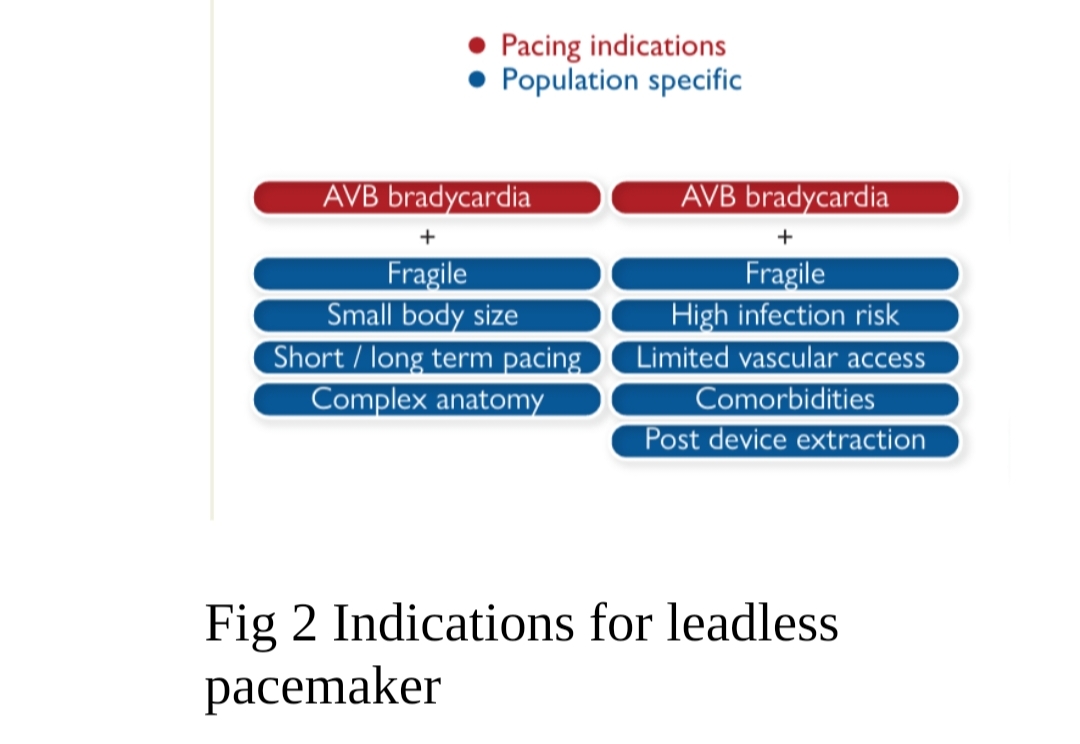
Leadless pacemakers are particularly beneficial in carefully selected patients where conventional pacemaker implantation may be technically difficult or associated with increased procedural risk. Common indications include specific group of patients with bradycardia as in Fig 2:
Elderly and frail patients
Bedridden or minimally ambulatory patients
Patients with difficult venous access
History of pacemaker pocket infection or device-related infection
Patients at high risk for lead-related complications
Chronic kidney disease and dialysis patients
Patients requiring minimally invasive cardiac rhythm management
Complex congenital heart disease pre and post-surgical management
Selected patients requiring physiological dual-chamber pacing
Because of their minimally invasive nature, leadless pacemakers are increasingly becoming an attractive option in complex, comorbid, and high-risk patients.
Case
Our patient was an elderly female with multiple longstanding medical comorbidities, including Type 2 Diabetes Mellitus, systemic hypertension, severe rheumatoid arthritis with fixed flexion deformities, and Acute Kidney Injury (AKI Stage II). Owing to advanced rheumatoid arthritis and severe musculoskeletal deformities, she had been largely bedridden for nearly two years with markedly restricted mobility and minimal ambulation, resulting in significant functional limitation and frailty.
She was brought to the emergency department with complaints of progressive breathlessness, generalised fatigue, reduced effort tolerance, and worsening orthopnea. Her symptoms had acutely worsened over a short duration, eventually progressing to severe respiratory distress. On presentation, she was found to be in acute pulmonary oedema with features of decompensated heart failure.
Clinical examination revealed significant bradycardia with hemodynamic instability. Electrocardiographic evaluation demonstrated complete heart block (third-degree atrioventricular block) with a slow escape rhythm, correlating with her clinical deterioration.
The patient’s overall clinical condition posed several unique therapeutic challenges. Her severe fixed flexion deformities secondary to rheumatoid arthritis made positioning extremely difficult for any invasive procedure. In addition, prolonged immobility, frailty, diabetes, renal dysfunction, and multiple systemic comorbidities significantly increased the procedural risk and the possibility of complications associated with conventional transvenous pacemaker implantation.
Given the urgent need for permanent pacing and the high-risk nature of conventional device implantation in this patient, the heart team decided to proceed with implantation of a dual-chamber leadless pacemaker system as a minimally invasive and safer alternative. The procedure was carefully planned with multidisciplinary coordination involving the cardiology and cardiac anaesthesia team.
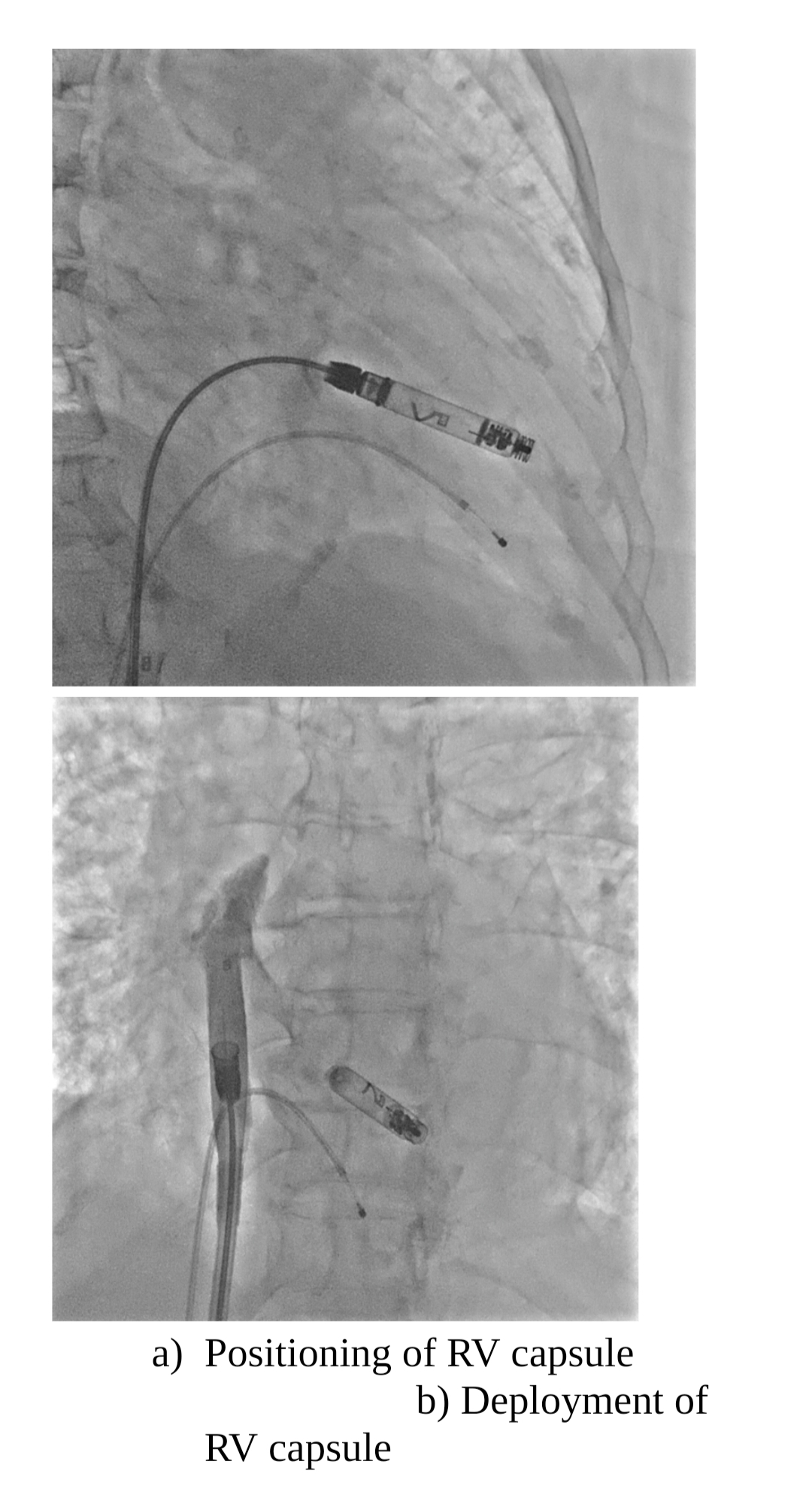
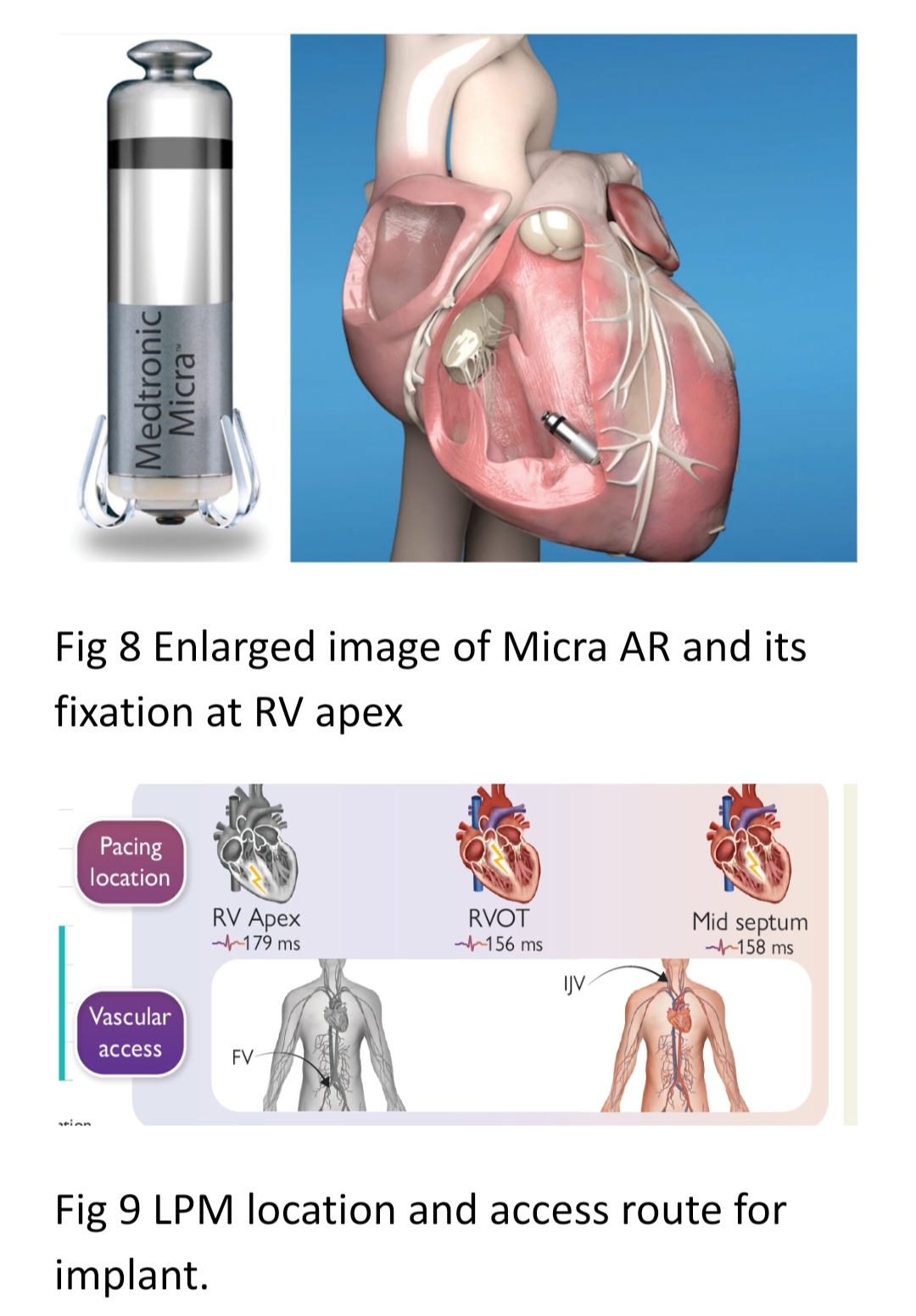
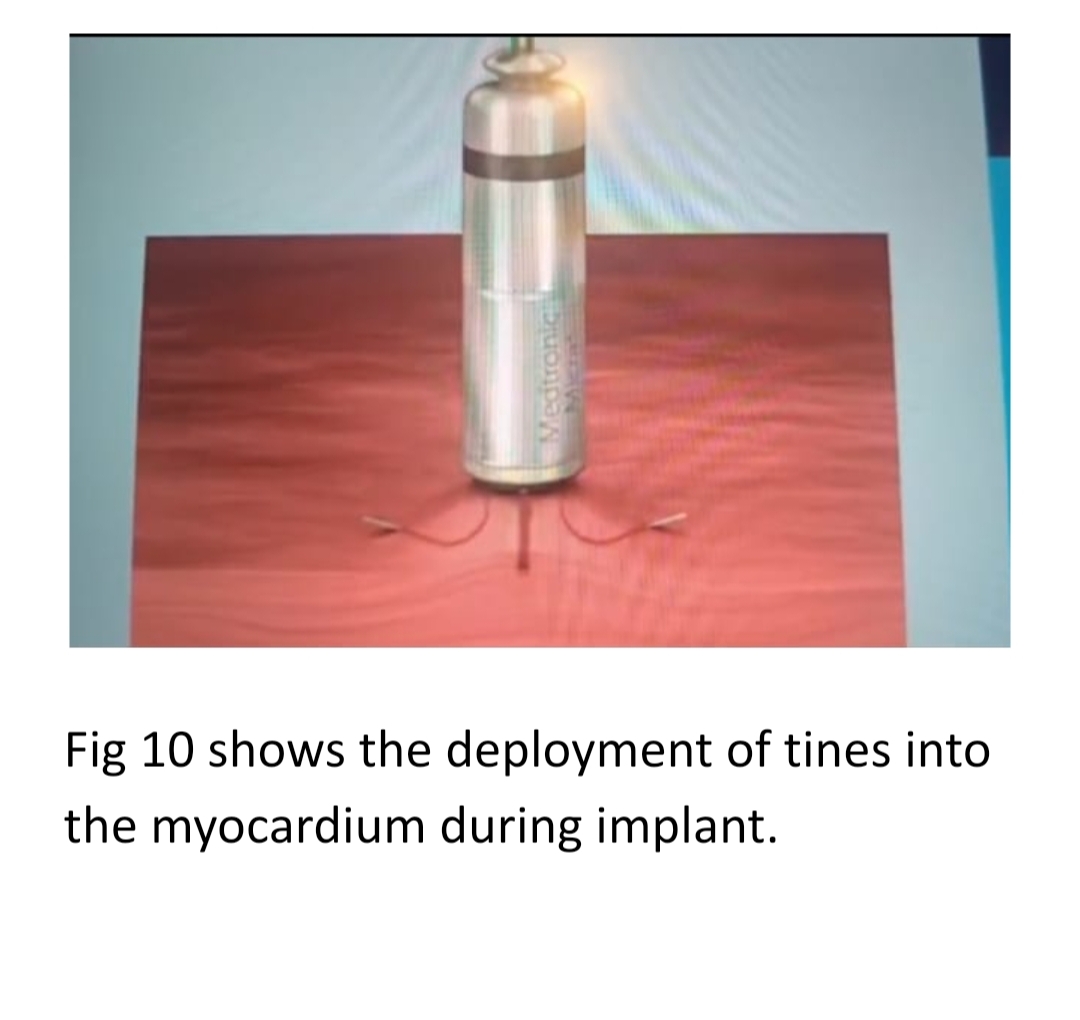
The procedure includes deployment of both ventricular and atrial capsules via large-bore access through either the femoral or internal jugular veins as in (fig 3,9) and is deployed via large soft, flexible specialized deflectable catheter systems with the help of fluoroscopy in the cath lab as described in fig 3. The capsule is implanted into the myocardium via flexible tines as in Micra fig 10, or via screws, as in the Avier system, either at the RV apical septum or the RV outflow tract.
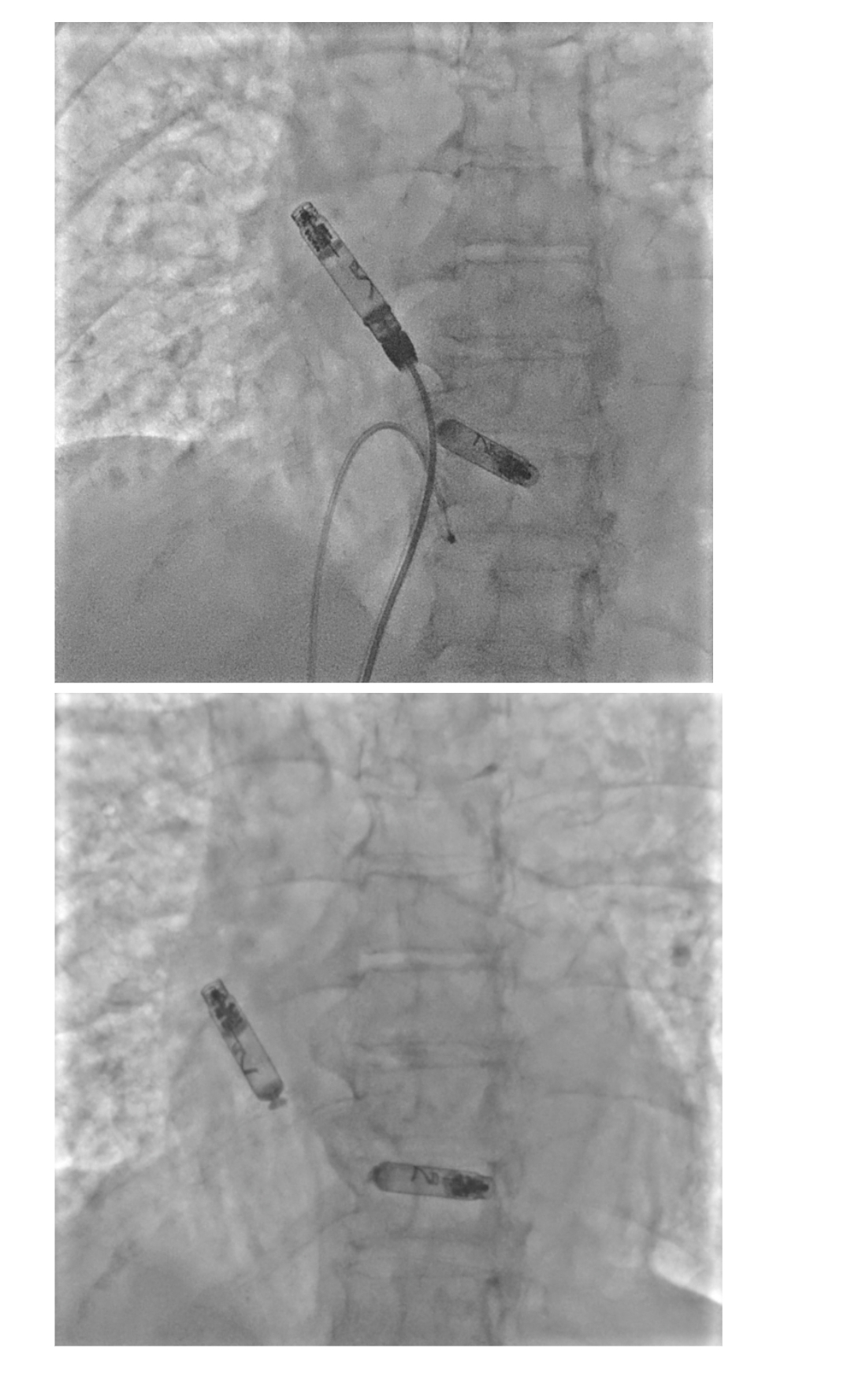
c) Deployment of RA capsule
d) Both RA and RV capsule in position.
Fig 3 Implantation of Leadless pacemaker
Importantly, PSG Hospitals had previously performed the first single-chamber leadless pacemaker implantation in Coimbatore (fig 7), reaffirming the institution’s continued leadership in adopting cutting-edge cardiac technologies and delivering advanced electrophysiology care.

The Future
Leadless pacing is here to stay. It is a rapidly evolving technology suitable for different pacing modalities and various patient populations. Long-term outcomes are promising, and complication rates decreased due to more experience and new developments. With several upcoming leadless technologies and improvements in currently available technologies, the future of pacing is beyond wires. Leadless cardiac defibrillators and cardiac resynchronization technologies are in the pipeline.
Dr R.B. Vidhyakar, MD, DM(CARDIO), CCDS, Fellowship in Cardiac Electrophysiology
Associate Professor, Department of Cardiology, PSGIMSR, CBE.














